Prof. Dr. med. Dietrich Tönnis
Sammlung wissenschaftlicher Arbeiten und Vorträge zur Orthopädie
Differences in the transiliac Osteotomies
© Prof. Dr. med. Dietrich Tönnis
By clicking on a figure an enlarged version of the figure will appear. At the end of the page you will find a PDF version of the paper.
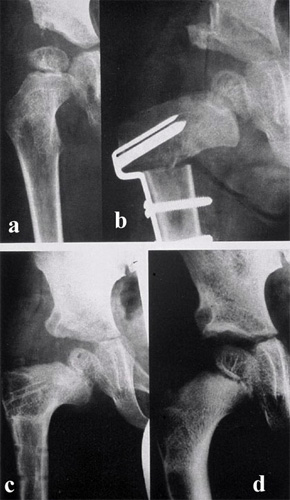 In my training in Berlin with Prof. A.N. Witt between 1960 and 1968 we started with these pictures of a complete transversal acetabuloplasty combined with an intertrochanteric varus osteotomy, and worked on the final form later in Dortmund (Fig. 1).
In my training in Berlin with Prof. A.N. Witt between 1960 and 1968 we started with these pictures of a complete transversal acetabuloplasty combined with an intertrochanteric varus osteotomy, and worked on the final form later in Dortmund (Fig. 1).
I would like to show you our technique and you will notice what is different (Fig. 2).
Own technique of acetabuloplasty
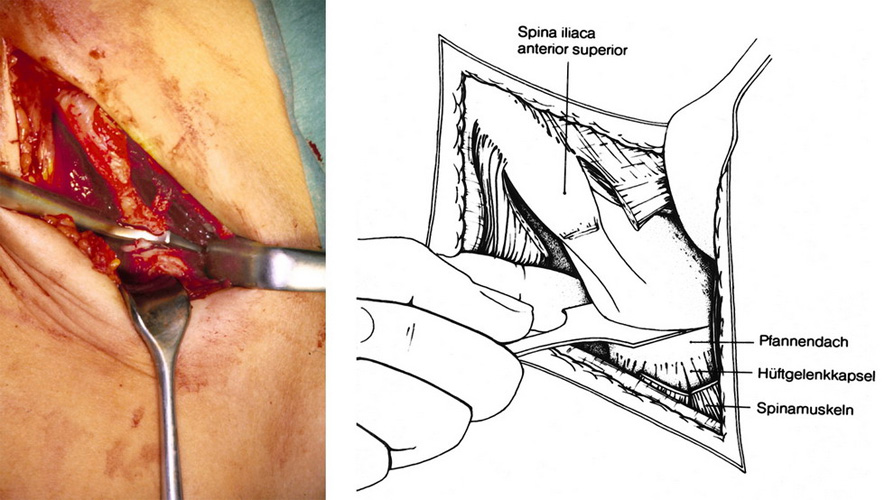 The inguinal incision is our preferred approach for open reductions of the hip and the transiliac osteotomy (Fig. 3). The scares are almost invisible. The incision starts from the anterior iliac crest to the groin parallel to the inguinal ligament. The tensor fasciae latae and the sartorius muscle are released ventrally. The detachment of the gluteus muscles in a length of 4-5 cm should be performed at the cartilage on top of the iliac crest, leaving a small stripe of cartilage at the muscle fibers to reinsert them here afterwards. The muscle fibers themselves should not be cut. The gluteus muscles then are carefully stripped subperiostally with a wide elevator down to the joint capsule and the lateral insertion of the rectus muscle tendon. This region should not be traumatized since the lateral growth centers are responsible for the growth of the acetabular rim till the end of growth.
The inguinal incision is our preferred approach for open reductions of the hip and the transiliac osteotomy (Fig. 3). The scares are almost invisible. The incision starts from the anterior iliac crest to the groin parallel to the inguinal ligament. The tensor fasciae latae and the sartorius muscle are released ventrally. The detachment of the gluteus muscles in a length of 4-5 cm should be performed at the cartilage on top of the iliac crest, leaving a small stripe of cartilage at the muscle fibers to reinsert them here afterwards. The muscle fibers themselves should not be cut. The gluteus muscles then are carefully stripped subperiostally with a wide elevator down to the joint capsule and the lateral insertion of the rectus muscle tendon. This region should not be traumatized since the lateral growth centers are responsible for the growth of the acetabular rim till the end of growth.
The inguinal ligament, abdominal muscles and iliacus muscle are also detached at the iliac crest, so that we see the blade of the osteotome anteriorly as it enters the inner side of the pelvis.
Then the glutaeus muscles above the capsule are stripped subperiostally back, up to the greater sciatic notch, until a finger can control the osteotomy as you see it here. The gluteus muscles should be retracted gently and by double rounded retractors. The superior gluteal nerve is close underneath this surface. A leasion causes limping.
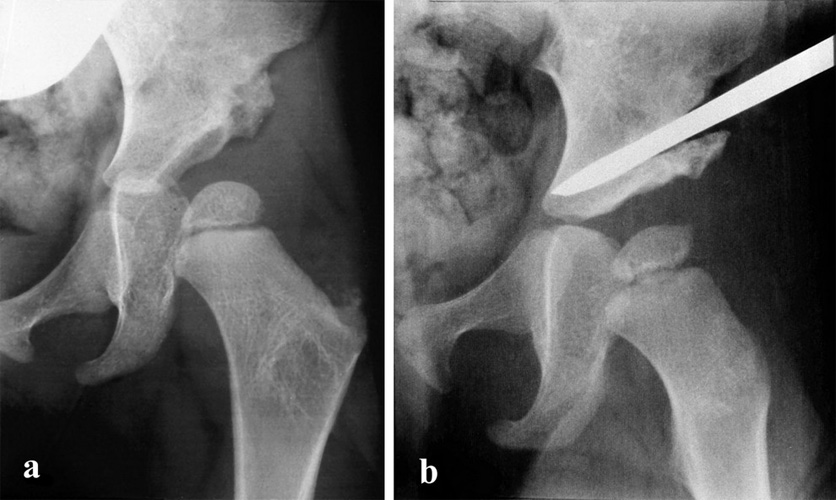
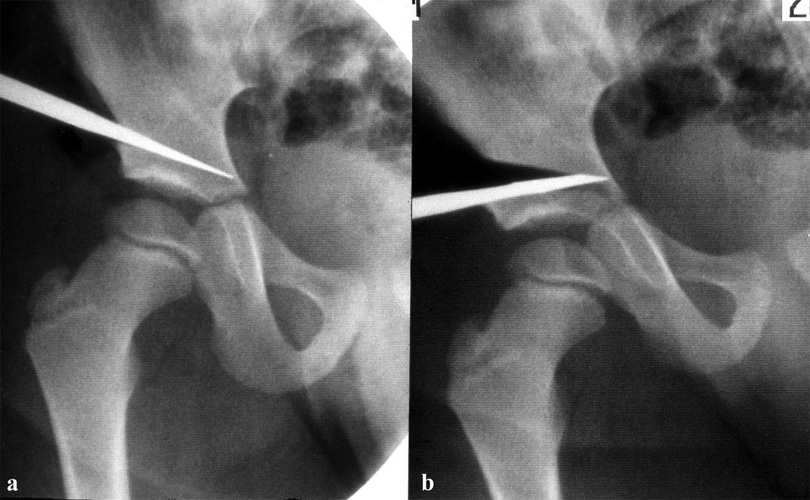
We osteotomize the acetabular roof 6-8 mm above the lateral acetabular margin using a flat Lexer osteotome (Fig. 4). The operation is performed on a radiolucent table. Using an image intensifier, the blade of the osteotome is driven toward the posterior rim of the triradiate cartilage. It should stop 5 mm before it. Anteriorly the blade passes through the anterior inferior iliac spine. Posteriorly it just enters the sciatic notch. There we check the blade position by palpation. The bone must be cut through completely from its anterior side back into the sciatic notch.
Then a good turn-down of the acetabular roof is possible. The hinge is placed by the 2 or 2,5 cm broad blade of the chisel, parallel to the posterior triradiate cartilage, at the medial side of the pelvic wing (Fig. 5).
The acetabular roof is turned down in the bone 5 millimeters apart of the triradiate cartilage. An angle of 5-10° should be achieved. 7 years later we find a perfect joint and coverage, here without a varus osteotomy. We shall come to this point.
 Our maximal angle of correction has been 50°. Here a deep frozen bone wedge from the bone bank has been pushed in medially and a peace of bone from the shortening osteotomy laterally (Fig. 6)
Our maximal angle of correction has been 50°. Here a deep frozen bone wedge from the bone bank has been pushed in medially and a peace of bone from the shortening osteotomy laterally (Fig. 6)
A hip spica in slight flexion of about 25° relieves the pressure on the femoral head.
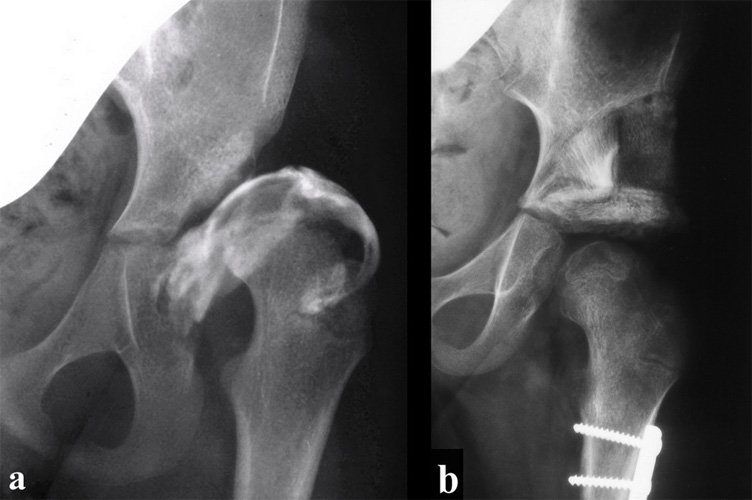
 When acetabuloplasty is combined with an open reduction and the dislocation was high, a subtrochantery shortening osteotomy is added to avoid ischemic necrosis of the femoral head (Fig. 7). A metal plate with 4 screws is sufficient since the child has to stay in a hip spica anyway and this is easier to perform than an intertrochanteric osteotomy.
When acetabuloplasty is combined with an open reduction and the dislocation was high, a subtrochantery shortening osteotomy is added to avoid ischemic necrosis of the femoral head (Fig. 7). A metal plate with 4 screws is sufficient since the child has to stay in a hip spica anyway and this is easier to perform than an intertrochanteric osteotomy.
First Long-Time Follow Up
| 90 hip joints in 67 children |
| Average age at operation: 3.6 years |
| Average age at follow-up: 15 years |
| No Pain or only occasional | 98% |
| No limitation of movement | |
| Trendelenburg limping negative | 71% |
Grade 1 |
15.5% |
Grade 3 |
13.5% |
In a first long-time follow-up of children with additional femoral varus osteotomies we reviewed in 1988 this material Tab.1. The clinical results are shown in Tab.2. They are good. Only the Trendelenburg limping was relatively high in grade 3 with 13.3%. Therefore my warnings in the beginning.
We investigated the children with our score of normal values and 4 deviation degrees (Tab. 3). We found for the different measurements percentages of normal and slightly pathological values mainly between 62 and 93%.
| Age (years/months) |
Normal value (mean) |
Grade 1 (normal) |
Grade 2 (mildly pathologic) |
Grade 3 (moderately pathologic |
Grade 4 (extremely pathologic) |
|---|---|---|---|---|---|
0/3 + 0/4 |
25 |
< 30 |
≥30–<35 |
≥35–<40 |
≥40 |
05 - 2/0 |
20 |
<25 |
≥25–<30 |
≥30–<35 |
≥35 |
x |
18 |
<23 |
≥23–<28 |
≥28–<33 |
≥33 |
x |
15 |
<20 |
≥20–<25 |
≥25–<30 |
≥30 |
x |
10 |
<15 |
≥15–<20 |
≥20–<25 |
≥25 |
Critical were only two measurements of the femoral neck, the epiphyseal index and the head-neck index (Tab. 4 and Tab. 5). They presented only 50% of normal and slightly pathological values.
| Acetabular angle (Ullmann, Sharp) | 93.2% |
| Acetabular angle (Weightbearing zone) | 62.0% |
| CE angle (Wiberg) | 82.0% |
| Migration percentage (Reimers) | 91.0% |
| Distance femoral head - teardrop figure | 87.6% |
| Neck-shaft angle | 86.7% |
| Antetorsion angle | 74.5% |
| Epiphyseal index (Eyre-Brook) | 50.0% |
| Head-neck index (Heymann-Herndon) | 47.7% |
| Epiphyseal KE angle | 76.5% |
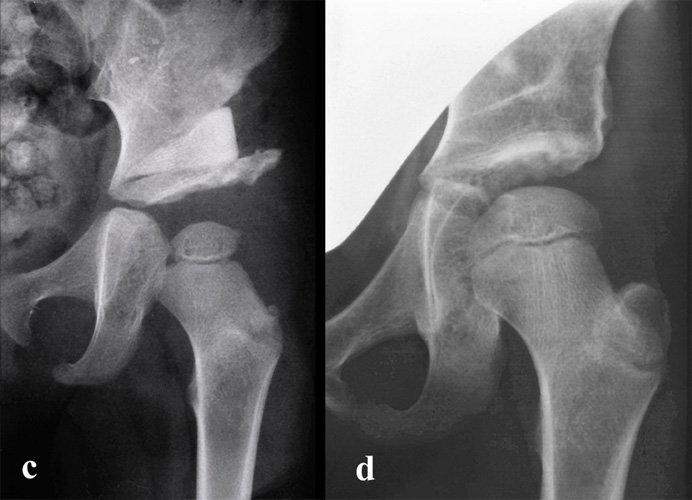
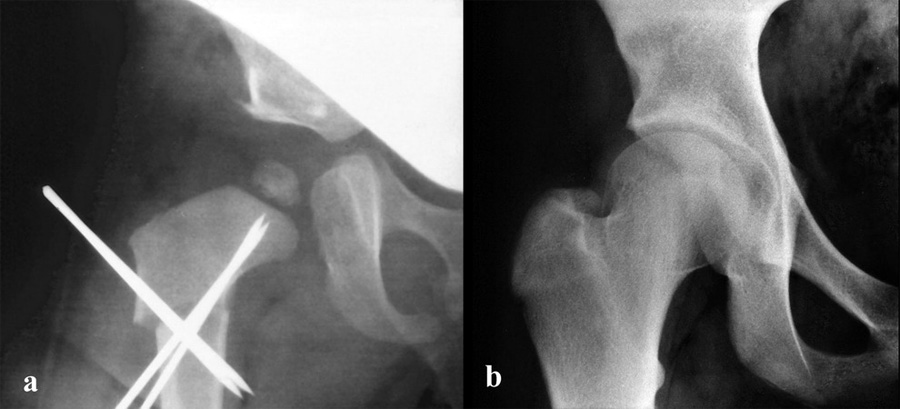 These patients had a tilt of the femoral head or it is called a subcapital coxa valga after varus osteotomy as you see it here (Fig. 8).
These patients had a tilt of the femoral head or it is called a subcapital coxa valga after varus osteotomy as you see it here (Fig. 8).
Ever since we avoided varus osteotomies.
Last Reinvestigation
A recent reinvestigation by Bonmann of actabuloplasties without varus osteotomy and with sterilized and deep frozen bone wedges in 52 hips have been perfect between 2 months and 9 years after operation. The femoral neck showed a normal development now in all joints.
The material operated between Jan. 1, 1991 and Dec. 31, 1992, reinvestigated later in the year 2000, so at a follow-up of 8-10 years consisted of 83 children with 125 operated joints. 91.2% of all patients were investigated.
| Angle | Before Op. | At follow-up | Valuation |
|---|---|---|---|
AC angle |
30° |
9.6° |
normal |
CE angle |
5.3° |
35.3° |
normal |
Ullmann-Sharp angle |
73 hips normal |
9 slightly pathological |
|
Harris hip score |
75 very good |
8 good |
|
Patients' opinion |
96.4% good and very good |
one not |
|
Tab. 6 shows the average of the different hip measurements at reinvestigation. The AC angle was corrected at operation from 30° to 9,6° in average, a normal angle, the CE angle from 5.3° to 35.3°, very good. Ullmann-Sharp angle in 73 hips normal, in 9 slightly pathological, The Harris hip score was very good in 75 hips, good in 8. The opinion of the patient was considered good and very good in 96.4% and not good in only one. These results and other physical ones are as good as wanted.
Conclusion
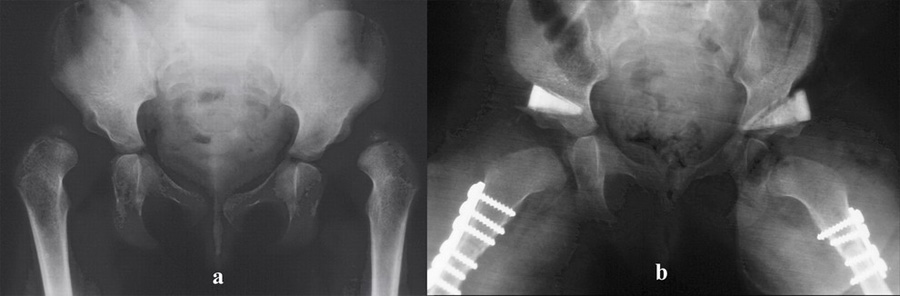
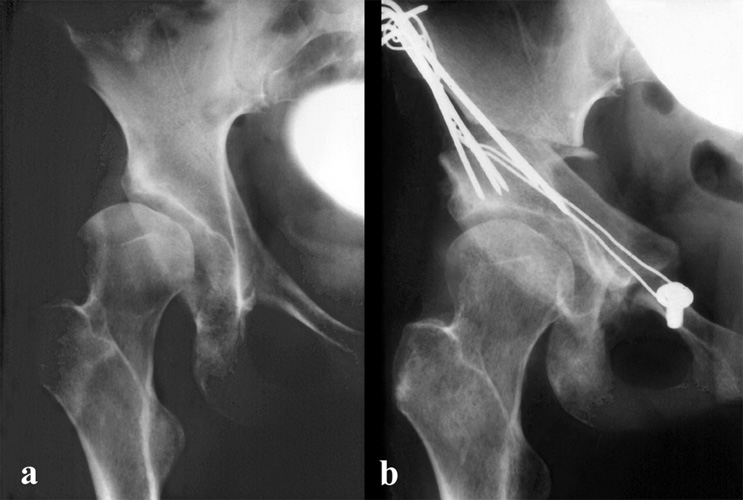 Later the whole acetabulum has to be rotated after disconecting it from the ligaments to the os pubis, os ischium and os ilium by a socalled triple pelvic osteotomy (Fig. 9).
Later the whole acetabulum has to be rotated after disconecting it from the ligaments to the os pubis, os ischium and os ilium by a socalled triple pelvic osteotomy (Fig. 9).
But this operation is more difficult and takes a longer time to recover. Residual dysplasias therefore should be treated as early as possible as we discussed it.
| Download | |
|---|---|
| Differences in the transiliac Osteotomies | PDF (1.4MB) |